
This month we cast a spotlight on articles, SurgeryU videos, and Journal of Minimally Invasive Gynecology (JMIG) article recommendations from the AAGL Robotics Special Interest Group (SIG) led by Chair, Erica Stockwell, DO, MBA, FACOG.
Access to SurgeryU and JMIG are two of the many benefits included in AAGL membership. The SurgeryU library features high-definition surgical videos by experts from around the world. JMIG presents cutting-edge, peer-reviewed research, clinical opinions, and case report articles by the brightest minds in gynecologic surgery.
SurgeryU video recommendations by our SIGs are available for public access for a limited time. The links to JMIG article recommendations are accessible by AAGL members only. For full access to SurgeryU, JMIG, CME programming, and member-only discounts on meetings, join AAGL today!

SIG Recommended SurgeryU Video #1:
Optimizing Surgeon Longevity: Ergonomics in Robotic Surgery
Ana Kouri, MD, Christina Lipscombe, MD, Jacqueline Wong, MD, Noor Abu-Alnadi, MD
This video describes the risk of physical injury to robotic surgeons by identifying common positioning and postural errors that lead to physical strain, and reviews optimal set up of the robotic console, bedside assistant, and uterine manipulator to decrease risk of work-related injury. Early adoption of optimal ergonomics prevents injuries and teaches trainees to integrate ergonomics into the foundation of their surgical skillset.
 Click Image to View Video
Click Image to View Video
SIG Recommended SurgeryU Video #2:
Utilizing Firefly Technology for Uterine Isthmocele Recognition and Excision: An Approach to Robotic Assisted Cesarean Scar Defect Repair
Melanie Evans, MD, Patrick Michael Weix, MD, PhD, Charles Herrin, MD, Orhan Bukulmez, MD
Firefly technology is an integrated benefit of the da Vinci robotic platform but is often under-utilized in benign gynecologic surgery. This video demonstrates how surgeons can utilize firefly fluorescent technology in a combined hysteroscopic and robotic assisted isthmocele repair for more accurate defect recognition and excision.
 Click Image to View Video
Click Image to View Video

JMIG Article Recommendation #1:
Jeremy Applebaum, MD, Edward K. Kim, MD, MPH, Joshua Ewy, MD, Leigh A. Humphries, MD, Divya K. Shah, MD, MME
This article examines the prevalence and accrual of 30-day postoperative complications by operative time for open myomectomy and minimally invasive myomectomy. The authors found that open myomectomy has a higher overall rate of composite, minor, and major complications compared to minimally invasive myomectomy.
JMIG Article Recommendation #2:
Anupama Bahadur, DNB, Bhawana Kumari Mallick, MD, Ayush Heda, MD, Anjali Pathak, DNB, Sakshi Heda, MS, Rajlaxmi Mundhra, MD
This RCT aims to evaluate the impact of the implementation of the enhanced recovery after surgery (ERAS) program in patients undergoing robotic hysterectomy for benign indications in comparison with conventional management. The combination of ERAS and robotic surgery improves patient outcomes, shortens hospital stays, and enhances postoperative recovery without increasing complications. This research serves as a pioneering effort in assessing the impact of ERAS on robotic hysterectomy for benign indications, providing valuable insights for future multicentric studies and supporting the integration of ERAS protocols to enhance patient outcomes and quality of life.

Shaping the Future of Robotic Surgery: Perspectives from Across the Globe
Robotics in Australia
by Mikhail Sarofim, BMed, MD, MS, FRANZCOG
I feel that our gynaecological careers could not have come at a better time. I recall reading a book about famous American pioneers, all born within a few years of each other: J.P. Morgan, Andrew Carnegie, John D. Rockefeller, and Henry Ford. Their collective success was partly attributed to the economic landscape of their time, which fostered unprecedented innovation and opportunity. This reminds me of the robotic era we are currently living in. Never has there been such a convergence of innovation, research, and support behind what is essentially a tool we use for surgery. I have the unique advantage of being able to use the three robotic systems approved by the Therapeutic Goods Administration (TGA), the medicine and therapeutic regulatory agency here in Australia.
The da Vinci by Intuitive, Versius by CMR Surgical, and HUGO-RAS by Medtronic are transforming the field of gynaecological surgery with their unique features and capabilities.
The da Vinci system has been a cornerstone in robotic surgery for years. Its robust design and intuitive interface have made it a preferred choice for many complex procedures. The da Vinci’s ability to offer high-definition 3D vision and enhanced precision allows surgeons to perform intricate surgeries with confidence. This system’s proven track record and continuous updates ensure it remains at the forefront of surgical innovation. Da Vinci is the Rolex of the robots. It is sleek, precise, and highly sought after. With that, it is also expensive. [figure 1]
 Figure 1
Figure 1
In contrast, the Versius system by CMR Surgical brings a fresh perspective with its ergonomic and compact design. This system is particularly beneficial in smaller operating rooms and for teams transitioning to robotic surgery. Versius is great for a lower-cost option. The Versius system is like a stylish, modern car that turns heads with its sleek design and innovative features. It offers a smooth, user-friendly experience and is a joy to drive. However, while it boasts impressive looks and comfort, it might not be as robust or reliable as some more established brands, occasionally requiring a bit more maintenance to keep it running at its best. [figure 2]
 Figure 2
Figure 2
The HUGO-RAS system by Medtronic came into the market with high expectations given it has rich parents. It emphasises flexibility and accessibility. Its modular design allows hospitals with varying budgets and needs to integrate robotic systems into their operating rooms. HUGO-RAS’s open-console architecture permits a more traditional laparoscopic setup while still benefiting from robotic precision. It is modular, like Versius; however, the arms are significantly larger and can often pose a threat to your assistants if you are reckless with your driving! [figure 3]
 Figure 3
Figure 3
Robotics in the United States
by Erica Stockwell, DO, MBA, FACOG
There are currently three robotic platforms that are Food and Drug Administration (FDA) approved for gynecologic surgery in the United States: Intuitive’s da Vinci system, Senhance by Asensus Surgical, and Anovo by Momentis. I am in a unique practice setting where I have access to all three of these platforms for direct patient care and will henceforth provide a quick overview of each.
Intuitive Surgical is certainly the behemoth in the room at a whopping 85% market share of the robotic surgery space. Their advanced technology and market penetrance has made the barrier to entry quite tough for other robotic companies. Intuitive’s latest splash to the market is the da Vinci 5. The da Vinci 5 enables force feedback technology, improved vision system, a greater range of motion and wide range of ergonomic settings for surgeon comfort, greater surgeon autonomy with console control, integrated media management, option for telepresence, and big data collection to enable future AI and machine learning. Operating on the da Vinci 5 for the first time after being so accustomed to the Xi felt like the first time stepping out of my Ford Explorer and driving a Tesla Model 3. I feel the updates have largely focused on improving patient safety and surgeon autonomy, as well as allowing for future software integration. Of course, the downside to all the bells and whistles, as mentioned previously, is the high price tag. [figure 4]
 Figure 4
Figure 4
Senhance by Asensus Surgical is a modular robot with open-platform architecture that uses familiar laparoscopic techniques and instrumentation. The company boasts augmented intelligence by providing haptic sensing, eye-tracking camera control, and a range of 3 mm and 5 mm reusable instruments. The transition from laparoscopy to Senhance is smooth for a surgeon who is proficient at laparoscopy but has a very different feel than other similar robotic platforms. [figure 5]
 Figure 5
Figure 5
Anovo by Momentis offers the first and only robotic platform for transvaginal surgery. At only 12 pounds, the robot itself is very small and portable, attaching to the table. The console is an open-platform concept that is agnostic to existing surgical equipment, thus decreasing overall cost. The instrument arms have humanoid articulation with wrist, elbow and shoulder movements. The robotic trocar is a single incision through the posterior cul-de-sac. Limitations of the platform include a limit on uterine size, inability to exchange arms, restricted endofactor profile, reliance on an assistant to drive the camera, and cumbersome uterine manipulation since the robot is docked between the legs. Momentis is very new to the market and has a way to go but is likely to continue to improve their technology over time. [figures 6a and 6b]
 Figures 6a &6b
Figures 6a &6b
A Competitive Landscape Driving Innovation
“Innovation is the ability to see change as an opportunity, not a threat.” – Steve Jobs
The introduction of the aforementioned robotic platforms has injected much-needed competition into a market historically dominated by the da Vinci system. This competition is beneficial for patients and the healthcare industry as a whole. For patients, this competition means better and more affordable access to state-of-the-art surgical care. Additionally, the diversity of robotic platforms encourages continuous technological advancements, which will no doubt grow exponentially.
From our unique vantage points, having utilized diverse systems, we see a bright future for robotic surgery. The blend of established excellence with innovative newcomers creates a dynamic environment where the primary beneficiary is the patient.
About the Authors:
Mikhail Sarofim, BMed, MD, MS, FRANZCOG
Erica Stockwell, DO, MBA, FACOG


Dr. Sarofim is a member of the AAGL and Associate Professor and Director at Eden Women’s Health in Australia.
Dr. Stockwell is Chair of the AAGL Robotics SIG and a Gynecologic Surgeon at AdventHealth in Celebration, Florida.

Pelvic Endometriosis with Right External Iliac Vein Involvement
Clinical History:
I had a 34-year-old, female patient that came to my office with a history of dysmenorrhea and chronic pelvic pain for the past 3 years. Previous treatments included nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives and dienogest, with partial relief. No history of significant trauma or surgeries. The patient presented with severe right lower abdominal and pelvic pain radiating to the right thigh, worsening during menstruation. The pain has been persistent and escalating over the past six months, significantly impacting her daily activities and quality of life. After stopping medical treatment to try to get pregnant the pain became excruciating, and she sought a specialist consultation at my office.
Clinical Examination:
On physical examination, the patient presented painful vaginal examination, with identification of a nodule in the retro cervical region, in addition to thickening of the uterosacral ligaments. Abdominal examination didn’t show anything remarkable. The diagnosis initially suggested was pelvic endometriosis with involvement of the vagina, uterosacral ligaments and possible intestinal endometriosis.
Image:
MRI confirmed extensive pelvic endometriosis invading bowel wall longitudinally for 2cm, uterosacral ligaments and left ovary (3,0 cm endometrioma). The unusual finding was a cystic endometriotic lesion involving the medial aspect of the right external iliac vein measuring 2,0 cm. The mass appeared to compress and invade superficially the vein.
Final Diagnosis:
Extensive pelvic endometriosis with a lesion compromising bowel, ovary, uterosacral ligaments and the right external iliac vein, leading to significant pain.
Surgical Intervention:
Robotic approach was performed (Image 1). Intraoperative findings confirmed extensive endometriotic implants involving the pelvic peritoneum, left ovary, bowel and cystic involvement of the right external iliac vein (Images 2 and 3). Pelvic excision of the endometriotic tissue, left oophoroplasty, and intestinal discoid resection were made. Careful dissection and removal of the endometriotic tissue compromising the vein was performed (Image 4).
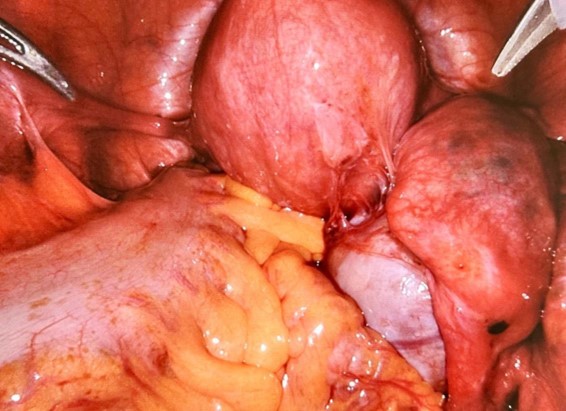 Image 1: Pelvic Initial View
Image 1: Pelvic Initial View
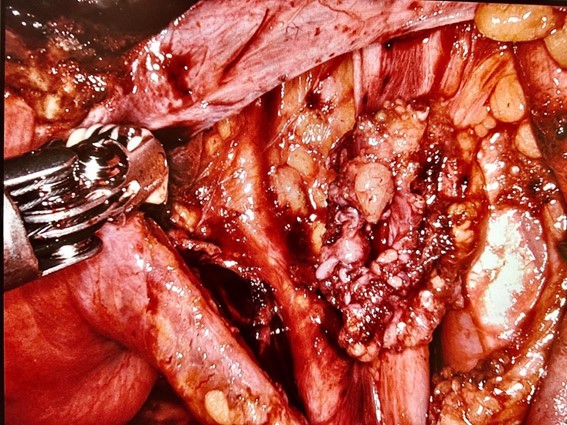 Image 2: Cystic Lesion Compromising the Right External Iliac Vein
Image 2: Cystic Lesion Compromising the Right External Iliac Vein
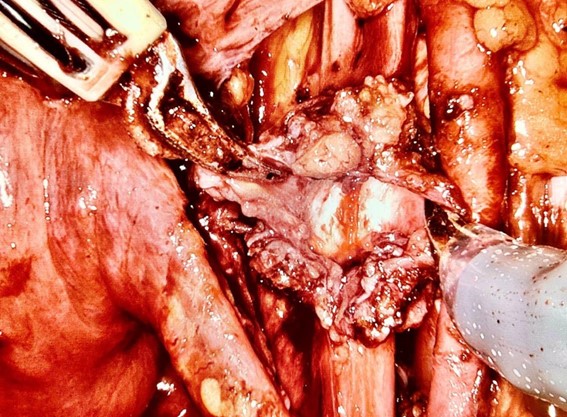 Image 3: Cystic Lesion Compromising the Right External Iliac Vein
Image 3: Cystic Lesion Compromising the Right External Iliac Vein
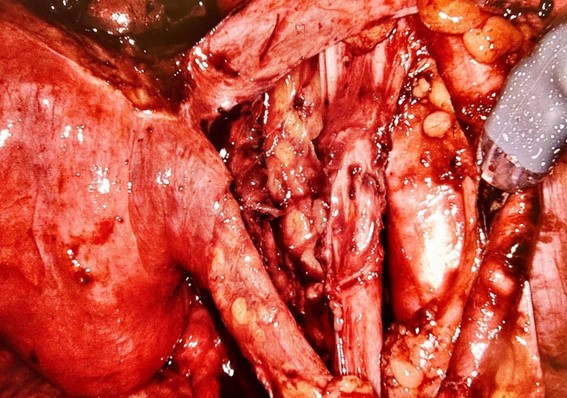 Image 4: Final View of the Right External Iliac Vein
Image 4: Final View of the Right External Iliac Vein
Outcome and Follow-Up:
After the surgery the patient experienced significant relief from pelvic pain and from the right thigh pain as well. Continued hormonal therapy and lifestyle modifications were advised.
Discussion:
This case highlights the complexity of endometriosis, particularly when it involves vital structures such as the external iliac vein. Endometriosis can cause significant morbidity. Interdisciplinary management, including gynecology and vascular surgery, is crucial for optimal patient outcomes. Early diagnosis and tailored treatment strategies can significantly improve quality of life for patients suffering from this debilitating condition.
About the Author:
Thiers Soares, Dr h, c., MD

Dr. Soares is Vice-Chair of the AAGL Robotic Special Interest Group and an endoscopic and robotic surgeon at Pedro Ernesto University Hospital and Cardoso Fontes Federal Hospital in Rio de Janeiro, Brazil.
The post Spotlight On: Robotics appeared first on NewsScope.