
This month we cast a spotlight on articles, SurgeryU videos, and Journal of Minimally Invasive Gynecology (JMIG) article recommendations from the AAGL Fibroids Special Interest Group (SIG) led by Chair, Kristen Pepin, MD, MPH.
Access to SurgeryU and JMIG are two of the many benefits included in AAGL membership. The SurgeryU library features high-definition surgical videos by experts from around the world. JMIG presents cutting-edge, peer-reviewed research, clinical opinions, and case report articles by the brightest minds in gynecologic surgery.
SurgeryU video recommendations by our SIGs are available for public access for a limited time. The links to JMIG article recommendations are accessible by AAGL members only. For full access to SurgeryU, JMIG, CME programming, and member-only discounts on meetings, join AAGL today!

What Do We Know About Trial of Labor After Myomectomy (TOLAM)?
Uterine fibroids are common benign tumors in reproductive-aged women. More patients are choosing uterine/fertility-preserving options for fibroids. (1) The BIG questions are what are we as surgeons counseling patients regarding the recommended mode of delivery in future pregnancies and who should be offered a trial of labor after myomectomy (TOLAM)? Obstetric providers rely on our operative report for guidance, so what should we be communicating and how can we predict the risk of uterine rupture in pregnancy?
Uterine rupture can be a catastrophic event during pregnancy with high rates of maternal and fetal morbidity and mortality. While there is robust literature regarding the risk of uterine rupture during a trial of labor after cesarean section (TOLAC), a trial of labor after myomectomy (TOLAM) has been much less studied and remains controversial. Although it may be tempting to recommend a pre-labor cesarean delivery to all patients after myomectomy, we should not forget the risk of future surgical morbidity, such as placenta accreta spectrum, which compound with increasing uterine incisions.
The largest study to date on uterine rupture after myomectomy includes a 2016 meta-analysis of 23 studies which found the overall rate of uterine rupture to be 0.6% in patients with history of myomectomy, but interestingly the rate was highest before the onset of labor (1.52%) compared to uterine ruptures occurring during trial of labor (0.47%). Thus, some have advocated to allow for a trial of labor after myomectomy given the uterine rupture risk is similar to TOLAC. (2)
Given myomectomies are performed with various surgical approaches and techniques, some studies have tried to examine whether these operative factors can help us predict risk of uterine rupture. Initial experience with laparoscopic myomectomy suggested there was a higher risk of uterine rupture compared to open myomectomy, which was thought to be from excessive diathermy and suturing technique. (3,4) However, as our technique and instrumentation improved, laparoscopic myomectomy was no longer found to have an increased risk of uterine rupture compared to the open approach in the hands of an expert surgeon. (5) Weibel et al. found that providers strongly rely upon entry into the endometrial cavity to decide whether to allow for TOLAM (6), however, there is no strong evidence to support this in the literature. The retrospective nature and small sample size of many of the available studies assessing features of a myomectomy, such as number, type, size of myomas; suture types used, and level of hemostasis limit the quality evidence on which providers can assess which of these factors increase the risk of rupture.
In terms of RF ablation of uterine fibroid, recent but ongoing data from ULTRA study showed successful pregnancy and vaginal delivery after this procedure. (7)
Thus, uterine rupture after myomectomy is rare but unpredictable. Evidence to help guide us in selecting appropriate candidates for TOLAM is lacking. We believe it is time for us to focus on more research efforts on TOLAM and try to figure out how to better identify risk factors and collaborate to provide better data.
References
- Myomectomy Market Size, Share & Trends Analysis Report By Type (Abdominal, Hysteroscopic, Laparoscopic), By Product (Laparoscopic Power Morcellators, Harmonic Scalpel, Laparoscopic Sealer), By Region, And Segment Forecasts, 2020 – 2027. Grand View Research. https://www.grandviewresearch.com/industry-analysis/myomectomy-market
- Gambacorti-Passerini Z, Gimovsky AC, Locatelli A, Berghella V. Trial of labor after myomectomy and uterine rupture: a systematic review. Acta Obstet Gynecol Scand 2016; 95: 724–734.
- Xiaoyi Wu, Wei Jiang, Huan Ju, Xuping Yi, and Congjian Xu. Characteristics of uterine rupture after laparoscopic surgery of the uterus: Clinical analysis of 10 cases and literature review. Journal of International Medical Research 2018, vol 46 (9) 3630-3639
- William H Parker, Jon Einarsson, Olav Istre, Jean-Bernard Dubuisson. Risk factors for uterine rupture after laparoscopic myomectomy. J Minim Invasive Gynecology 2010 Sep-Oct, 17 (5): 551-4
- J Claeyes, I Hellendoorn. T Hamerlynck, J Bosteels. S Weyers. The risk of uterine rupture after myomectomy: a systematic review of the literature. Gynecolog Surg (2014) 11: 197-206
- Weibel HS, Jarcevic R, Gagnon R, Tulandi T. Perspectives of obstetricians on labour and delivery after abdominal or laparoscopic myomectomy. J Obstet Gynaecol Can. 2014 Feb;36(2):128-32. doi: 10.1016/s1701-2163(15)30658-7. PMID: 24518911
- Allen, Antoinette MD; Schembri, Michael BS; Parvataneni, Ram MD, MPH; Waetjen, L. Elaine MD; Varon, Shira MD; Salamat-Saberi, Naghmeh MD; Tassone, Shawn MD, PhD; Williams, Nicole MD; Kho, Kimberly A. MD, MPH; Jacoby, Vanessa L. MD, MAS. Pregnancy Outcomes After Laparoscopic Radiofrequency Ablation of Uterine Leiomyomas Compared With Myomectomy. Obstetrics & Gynecology 143(5):p 612-618, May 2024
About the Authors
Naghmeh Salamat Saberi, MD
Rebecca Post, MD
Alison Sherman Brown, MD


Dr. Saberi (senior author) is Clinical Professor of OB/GYN at the University of California Irvine in Irvine, California.
Dr. Post is Assistant Clinical Professor at the University of California Irvine in Irvine, California.
Dr. Brown is a fellow at the University of California Irvine in Irvine, California.

NEW! SIG Recommended SurgeryU Video #1:
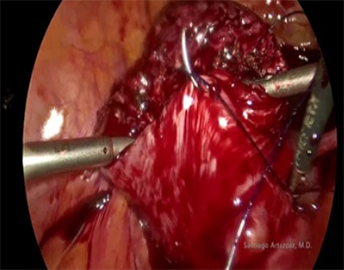
Myoma Screw in Laparoscopic Myomectomy
By Santiago Artazcoz, MD
Laparoscopic myomectomy can be one of the most complex surgeries in minimally invasive gynecological surgery. The limited space to maneuver within the pelvis, the alteration of pelvic anatomy, and the excessive bleeding that occurs during myomectomy are sometimes obstacles that lead surgeons to prefer performing the myomectomy openly. Good surgical technique can help us overcome these difficulties. The use of the myoma screw is an excellent tool for constant traction on the myoma, thereby finding the correct cleavage plane to perform a faster surgery with less bleeding. The technique of myomectomy is very important to prevent excessive bleeding; the assistant’s compression on the myomectomy bed and effective suturing are the next steps to ensure effective hemostasis. Good uterine reconstruction is essential to prevent complications in the event of a future pregnancy.
 Click Image to View Video
Click Image to View Video
About the Author
Santiago Artazcoz, MD
 Dr. Artazcoz is a member of the AAGL Fibroids SIG, Secretary for the Argentine Society of Endometriosis, and a MIGS Surgeon from Argentina. He is currently joining Mount Sinai as a PGY-1 to restart residency and practice as a MIGS specialist in the US.
Dr. Artazcoz is a member of the AAGL Fibroids SIG, Secretary for the Argentine Society of Endometriosis, and a MIGS Surgeon from Argentina. He is currently joining Mount Sinai as a PGY-1 to restart residency and practice as a MIGS specialist in the US.
SIG Recommended SurgeryU Video #2:
Laparoscopic Myomectomy for a Large Incarcerated Posterior Myoma
By Elaine M Jaworski, MD
The case is well presented. I liked the surgery due to the difficulty of the myoma’s location and the techniques used for ligating the uterine arteries. It also highlights the importance of understanding different approaches to the retroperitoneum, which are very useful in cases where the anatomy is altered.
The uterine reconstruction seemed very appropriate to me, with the suturing done correctly to avoid leaving dead spaces between the tissues.
 Click Image to View Video
Click Image to View Video
SIG Recommended SurgeryU Video #3:
Prostaglandin Injection for Myoma Eversion (PRIME): A Novel Approach to Type 2 Myomas
By Lulu Yu, MD, MPHS
Just like the explanation in the JMIG work, I found it interesting to watch the surgery video after reading the article. I think that the injection of prostaglandin can be a good resource for this type of myomas.
 Click Image to View Video
Click Image to View Video
SIG Recommended SurgeryU Video #4:
Robotic Myomectomy for Pararectal Myoma Arising from the Uterosacral Ligament
By Natalie E. Rivera
The most difficult cases are often the most attractive. In this case, the use of the robot allows for better control of instruments in more complex locations. The choice of the approach outside the infundibulopelvic ligament is appropriate.
 Click Image to View Video
Click Image to View Video

JMIG Article Recommendation #1:
Prostaglandin Injection for Myoma Expulsion (PRIME): Case Series of a Novel Approach to Hysteroscopic Resection of FIGO Type 2 Myomas
Sarah C. Cromack, MD, Lulu Yu, MD, and Magdy P. Milad, MD, MS
FIGO type 2 Myomas have always been a challenge for the gynecological surgeon. They are often characterized by being highly symptomatic and difficult to fully resect in a single procedure. Prostaglandin injection during hysteroscopy may represents a novel, safe, and rapid option to facilitate the expulsion of the fibroid, thereby achieving its resection in a single surgical session. Although the presented series is small and lack of a control comparator group, it may be a good start for designing further studies that explore the utility and safety of this tool, not only by increasing the sample size but also by designing comparative studies of this intervention with other available options.
JMIG Article Recommendation #2:
Determination of Whole Blood Loss From Minimally Invasive Myomectomy Using a Standardized Formula: A Pilot Study
Marisa Gigg, MD, Kathryn Goldrath, MD, Alexandra Havard, MD, Anissa V. Nguyen, MPH, Lorna Kwan, MPH, Ram Parvataneni, MD, MPH, Sukrant Mehta, MD, Alexander Chiang, MD, Valentina Rodriguez, MD, and Jacqueline Fahey, MD
Postoperative anemia can delay patient recovery, increase hospital discharge time, and raise transfusion requirements. Accurately estimating blood loss allows us to identify patients who will require more extensive hemostatic measures and closer monitoring, considering that perioperative blood loss is greater than the estimated intraoperative blood loss. The application of this equation provides evidence that exists a continued blood loss post myometrial bed closure.
JMIG Article Recommendation #3:
Feasibility and Perioperative Outcomes of Minimally Invasive Higher Order Myomectomy
Marie-Claire Leaf, MD, Alexandra Lombardo, MS, Julia J. Wainger, MD, MPH, Mostafa A. Borahay, MD, PhD, Anja Frost, MD, Kristin Patzkowsky, MD, Karen C. Wang, MD, Harold Wu, MD, and Khara Simpson, MD
Minimally invasive higher-order myomectomy is a feasible option for patients with a large fibroid burden. Patients with 10 or more fibroids removed had higher estimated blood loss, higher incidence of hemorrhage >1000 mL, and higher use of cell saver transfusion than those with fewer than 10 fibroids removed. The conversion to laparotomy rate and overall complication rate did not differ significantly between patients with fewer than 10 fibroids removed and those with ten or more fibroids removed. The average operating time for higher-order myomectomy was longer than for lower-order myomectomy. The odds of requiring another surgery for fibroids were significantly higher for those undergoing higher-order myomectomy compared to lower-order myomectomy. In conclusion, in skilled hands, it is feasible to do minimal access myomectomy for a large fibroid burden.

Use of AI and Machine Learning in the Management of Uterine Leiomyomas
Uterine fibroids are a common gynecological condition affecting millions worldwide. The use of artificial intelligence (AI) and machine learning has shown promising results in both diagnostic capabilities and prediction of successful treatment. The emergence of AI-based research over the past few years has led researchers to explore the power AI has and its potential effects on management of uterine fibroids. AI algorithms can analyze large amounts of clinical data as well as identify patterns and predict outcomes to ultimately guide treatment decisions. By applying the abilities of AI and machine learning, gynecologists can better characterize the radiological findings of uterine fibroids and develop appropriate and personalized treatment plans that are tailored to each patient’s unique characteristics and needs.
With a growing number of physicians and institutions understanding the utility and advantages of incorporating machine learning and AI into the clinical setting, technology companies and startups are partnering with physician scientists and researchers to push the envelope in AI and machine learning research. We have engaged in such partnerships as well and therefore can share our experience with other obstetricians and gynecologists. This collaboration allows for the translation of cutting-edge AI innovations into practical clinical applications that can directly benefit patients.
Current literature focuses on several management points regarding uterine fibroids mainly exploring AI-based diagnosis1-2 and prediction of successful treatment of fibroids.3-8 Other areas of exploration include machine learning for differentiation of benign versus malignant disease9-16 as well as AI guided surgical simulation for gynecological surgery including surgical management of uterine fibroids.17,18 When applied specifically to the management of uterine fibroids, machine learning models have shown promising results. Several studies reported high prediction capabilities of successful high-intensity focused ultrasound (HIFU) guided ablation of uterine fibroids, based on MRI parameters (area under the curve (AUC) of 0.89-0.95).3-6 Similar success rates were reported in differentiating benign from malignant disease, with excellent diagnostic efficacy, with reported AUC reaching 0.97.8,10
One major challenge is the lack of standardized data collection and reporting across different healthcare institutions, leading to variability in data quality and model performance. For example, while some institutions choose to report the finding of uterine fibroids based on FIGO criteria, others may simply recognize their presence with or without describing their size or other radiological characteristics.
AI and machine learning have the potential to revolutionize the management of uterine fibroids, offering personalized and precise treatment options for women with this condition. By advancing research in this field, we can improve the outcomes and quality of life for women affected by uterine fibroids, ultimately transforming the landscape of women’s health and gynecological care.
References
- Lombardi A, Arezzo F, Di Sciascio E, Ardito C, Mongelli M, Di Lillo N, Fascilla FD, Silvestris E, Kardhashi A, Putino C, Cazzolla A, Loizzi V, Cazzato G, Cormio G, Di Noia T. A human-interpretable machine learning pipeline based on ultrasound to support leiomyosarcoma diagnosis. Artif Intell Med. 2023 Dec;146:102697. doi: 10.1016/j.artmed.2023.102697. Epub 2023 Nov 3. PMID: 38042596.
- Yang T, Yuan L, Li P, Liu P. Real-Time Automatic Assisted Detection of Uterine Fibroid in Ultrasound Images Using a Deep Learning Detector. Ultrasound Med Biol. 2023;49(7):1616-1626. doi:10.1016/j.ultrasmedbio.2023.03.013
- Akpinar E, Bayrak OC, Nadarajan C, Müslümanoğlu MH, Nguyen MD, Keserci B. Role of machine learning algorithms in predicting the treatment outcome of uterine fibroids using high-intensity focused ultrasound ablation with an immediate nonperfused volume ratio of at least 90. Eur Rev Med Pharmacol Sci. 2022;26(22):8376-8394. doi:10.26355/eurrev_202211_30373
- Zhang J, Yang C, Gong C, Zhou Y, Li C, Li F. Magnetic resonance imaging parameter-based machine learning for prognosis prediction of high-intensity focused ultrasound ablation of uterine fibroids. Int J Hyperthermia. 2022;39(1):835-846. doi:10.1080/02656736.2022.2090622
- Zheng Y, Chen L, Liu M, Wu J, Yu R, Lv F. Prediction of Clinical Outcome for High-Intensity Focused Ultrasound Ablation of Uterine Leiomyomas Using Multiparametric MRI Radiomics-Based Machine Leaning Model. Front Oncol. 2021 Sep 10;11:618604. doi: 10.3389/fonc.2021.618604. PMID: 34567999; PMCID: PMC8461183.
- Li C, He Z, Lv F, et al. An interpretable MRI-based radiomics model predicting the prognosis of high-intensity focused ultrasound ablation of uterine fibroids. Insights Imaging. 2023;14(1):129. Published 2023 Jul 19. doi:10.1186/s13244-023-01445-2
- Slotman DJ, Bartels LW, Zijlstra A, et al. Diffusion-weighted MRI with deep learning for visualizing treatment results of MR-guided HIFU ablation of uterine fibroids. Eur Radiol. 2023;33(6):4178-4188. doi:10.1007/s00330-022-09294-1
- Dai M, Liu Y, Hu Y, et al. Combining multiparametric MRI features-based transfer learning and clinical parameters: application of machine learning for the differentiation of uterine sarcomas from atypical leiomyomas. Eur Radiol. 2022;32(11):7988-7997. doi:10.1007/s00330-022-08783-7
- Lombardi A, Arezzo F, Di Sciascio E, et al. A human-interpretable machine learning pipeline based on ultrasound to support leiomyosarcoma diagnosis. Artif Intell Med. 2023;146:102697. doi:10.1016/j.artmed.2023.102697
- Nakagawa M, Nakaura T, Namimoto T, et al. A multiparametric MRI-based machine learning to distinguish between uterine sarcoma and benign leiomyoma: comparison with 18F-FDG PET/CT. Clin Radiol. 2019;74(2):167.e1-167.e7. doi:10.1016/j.crad.2018.10.010
- Nakagawa M, Nakaura T, Namimoto T, et al. Machine Learning to Differentiate T2-Weighted Hyperintense Uterine Leiomyomas from Uterine Sarcomas by Utilizing Multiparametric Magnetic Resonance Quantitative Imaging Features. Acad Radiol. 2019;26(10):1390-1399. doi:10.1016/j.acra.2018.11.014
- Santoro M, Zybin V, Coada CA, et al. Machine Learning Applied to Pre-Operative Computed-Tomography-Based Radiomic Features Can Accurately Differentiate Uterine Leiomyoma from Leiomyosarcoma: A Pilot Study. Cancers (Basel). 2024;16(8):1570. Published 2024 Apr 19. doi:10.3390/cancers16081570
- Malek M, Gity M, Alidoosti A, et al. A machine learning approach for distinguishing uterine sarcoma from leiomyomas based on perfusion weighted MRI parameters. Eur J Radiol. 2019;110:203-211. doi:10.1016/j.ejrad.2018.11.009
- Malek M, Tabibian E, Rahimi Dehgolan M, et al. A Diagnostic Algorithm using Multi-parametric MRI to Differentiate Benign from Malignant Myometrial Tumors: Machine-Learning Method. Sci Rep. 2020;10(1):7404. Published 2020 May 4. doi:10.1038/s41598-020-64285-w
- Wang T, Gong J, Li Q, et al. A combined radiomics and clinical variables model for prediction of malignancy in T2 hyperintense uterine mesenchymal tumors on MRI. Eur Radiol. 2021;31(8):6125-6135. doi:10.1007/s00330-020-07678-9
- Winkler-Schwartz A, Bissonnette V, Mirchi N, Ponnudurai N, Yilmaz R, Ledwos N, et al. Artificial intelligence in medical education: best practices using machine learning to assess surgical expertise in virtual reality simulation. 2019;76(6):1681–90. doi: 10.1016/j.jsurg.2019.05.015
- Hung AJ, Chen J, Gill ISJJS. Automated performance metrics and machine learning algorithms to measure surgeon performance and anticipate clinical outcomes in robotic surgery. 2018;153(8):770–1. doi: 10.1001/jamasurg.2018.1512
About the Authors
Itamar D. Futterman, MD
Scott Chudnoff MD, MSc


Dr. Futterman is a physician in the Maternal Fetal Medicine Department at Maimonides Health in New York City, New York.
Dr. Chudnoff is Vice Chair of the AAGL Fibroids SIG and Chair of Obstetrics & Gynecology and Women’s Health at Maimonides Health in New York City, New York.

Robotic Excision of Disseminated Peritoneal Leiomyomatosis
Power morcellation was a common practice for tissue extraction following laparoscopic myomectomy and hysterectomy until the 2014 US Food and Drug Administration (FDA) warning statement regarding power morcellation was released (1). One of the unintended consequences of uncontained power morcellation was the development of disseminated peritoneal leiomyomatosis (DPL), or parasitic leiomyomas. The incidence of DPL after laparoscopic morcellation is relatively low at 0.12-0.95% (2). Despite this, it is still important to be able to recognize the diagnosis and be able to provide minimally invasive surgical treatments.
We present a case of a 36-year-old gravida 0 with a history of a robot-assisted laparoscopic myomectomy with uncontained power morcellation 5 years prior. She presented with an enlarging left upper quadrant (LUQ) mass. A pelvic MRI showed a multi-fibroid uterus with multiple enhancing masses throughout the peritoneal cavity with similar imaging characteristics to uterine leiomyomas. About 10 extrauterine fibroids were mapped out on MRI and located in the upper abdomen and pelvis, near bowel, diaphragm, bladder and umbilicus. There was an additional 5.3cm mass in the left anterior abdominal wall between the internal and external oblique muscles. The planned procedure was a robot-assisted excision of parasitic myomas and myomectomy of 5 intramural/subserosal fibroids. The patient was counseled on the risks and benefits of open vs minimally invasive myomectomy with contained manual tissue extraction.
First a diagnostic laparoscopy was performed with initial entry into Palmer’s point. For a hybrid surgery involving the pelvis and upper abdomen, strategic port placement is key to ensure optimal access to the abdominal wall and pelvic myomas. To avoid the umbilical myoma, the camera was positioned supraumbilically and a modified M configuration was used. Camera port hopping was performed to facilitate multi-quadrant visualization. We began with identifying each of the 10 extrauterine fibroids that was previously mapped on MRI. The fibroids were grasped with a tenaculum, creating tension away from adjacent anatomy to minimize the risk of damage or thermal spread. Given the large feeding vessels from the omentum or mesentery, the use of a robotic vessel sealer was used. For myomas attached to the retroperitoneum and mesentery, it was crucial to identify vital surrounding structures such as the ureter, bowel and external iliac vessels.
The LUQ abdominal wall myoma (located between the external and internal oblique muscles) was approached from intraperitoneally to avoid a separate skin incision. The bedside assistant applied downward abdominal pressure to assist with identifying the location of the mass and its borders. A longitudinal incision into the layers of the abdominal wall was made until the fibroid was reached. Enucleation was performed to remove the mass from the abdominal wall. The fascial defect was inspected, and a multilayer tension-free closure was performed. The internal and transversalis fascia were reapproximated with a 0 running barbed suture. Then the posterior rectus sheath was closed separately. Once all the myomas were removed, the abdomen was inspected, and the small bowel was run from the terminal ileum to the ligament of Treitz. The intrauterine myomectomy was performed in the usual fashion. A total of 15 fibroid specimens were strung on a suture and placed in a containment bag for cold knife tissue extraction in the usual fashion.
References
- US Food and Drug Administration. UPDATED laparoscopic uterine power morcellation in hysterectomy and myomectomy: FDA safety communication. Silver Spring (MD): FDA;2014. https://wayback.archiveit.org/7993/20170404182209/https:/www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm424443.htm
- Van der Meulen JF, Pijnenborg JMA, Boomsma CM, Verberg MF, Geomini PM, Bongers MY. Parasitic myoma after laparoscopic morcellation: a systematic review of the literature. BJOG. 2016 Jan;123(1):69-75.
- Uterine Morcellation for Presumed Leiomyomas. ACOG Committee Opinion No. 882, March 2021.
- Kriplani I, Kriplani A, Sharma S, Sodhi M, Jain N. Laparoscopic management of disseminated peritoneal leiomyomatosis. J Minim Invasive Gynecol. 2023 Jun;30(6):443-444.
- Tan-Kim J, Hartzell KA, Reinsch CS, O’Day CH, Kennedy JS, Menefee SA, Harrison TAA. Uterine sarcoma and parasitic myomas after laparoscopic hysterectomy with power morcellation. Am J Obstet Gynecol. 2015 May;212(5):594.
About the Author
Jin Hee Kim, MD

Dr. Kim is a member of the AAGL Fibroids SIG and Associate Professor of Minimally Invasive Gynecologic Surgery, Department of Obstetrics and Gynecology at Columbia University Irving Medical Center in New York, New York.
The post Spotlight On: Fibroids appeared first on NewsScope.